The Latest In Controlling OR Heat Loss
-
Printer Friendly|#| Trackback
Keeping patients warm in the operating room can be a challenge. On call two weekends ago I had an 'Aha' moment--give them knit caps! Below is the protype--a scullcap made from 6 inch stockinette.
[note: this photo was taken with an iPhone!]
Tool of the Trade: Lidocaine
-
Printer Friendly|#| Trackback
Dr. Wes' post on the proper way to inject lidocaine got me to thinking about how I do it and I think I have some tips to share, too. I inject lidocaine in people's back while they're in labor, in their groins, necks, and arm pits when I do blocks, and of course in their hands and arms when I place IV's. (I inject it into their IV's, too, but there's no trick to that, really.)
When I have time, I like to add about a one fourth volume of bicarbonate to the lidocaine I'm injecting. (This doesn't work with bupivicaine as it will cause it to precipitate out.) I've testing this on myself, on nurses in labor, and in patients in labor and I am convinced this removes most of the burning sensation that comes with injecting lidocaine.
After having selected my injection site and cleaned it (with alcohol, betadine, chloraprep, duraprep, etc.) I wait for the prep to dry so that the prepping agent doesn't cause any stinging. I place a drop of lidocaine on the skin and insert the needle through the drop of lidocaine to make contact with the skin (after warning the patient, of course). This works, not because it numbs the skin under the drop (you need a eutectic mixture of local anesthetics for that) but because it caries some lidocaine in on the tip of the needle. I inject while inserting the needle intradermally. You should inject slowly, advance slowly, and see a skin wheal if it's truly an intradermal injection. This is easiest on horizontal surfaces but can also be done on a vertical surface like a back. In my opinion the wrong way to do inject lidocaine is the way tuberculin skin test are often placed: jab in the tiny needle (ouch!) inject the antigen quickly (ouch!).
When I watch trainees inject lidocaine I often see them stop to aspirate to make sure they're not in a blood vessel. This is unnecessary a) if you keep the tip of the needle moving and b) because the total dose of lidocaine in the 3cc syringe is not enough to cause toxicity even if injected intravascularly. We now return you to your regularly scheduled programming...
Nothing can stand between me and my bluegrass
-
Printer Friendly|#| Trackback
On call at the hospital today. The work is done and we're getting ready to order Chinese food. Time for some computer work and bluegrass. But wait! The hospital has decided to block XM streams!
Thank you iTunes: Bluegrass Radio 128 kbps 100 Percent Pure Acoustic Bluegrass
Life is good (again).
Safety Tip: Nerve Block Needle Disposal
-
Printer Friendly|#| Trackback
I most commonly use a 2 inch B-bevel insulated needle for nerve blocks. It is often not convenient to dispose of the block needle right away after completing the block, so I started placing it in the barrel of the empty syringe from the plunger side and holding it in place with by depressing the plunger. Like this:

Safer for myself and my assistant (when I have an assistant).
YouTube: Site-Rite Instructional Video
-
Printer Friendly|#| Trackback
The AHRQ published Making Health Care Safer: A Critical Analysis of Patient Safety Practices in 2001. Chapter 21 deals with Ultrasound Guidance of Central Vein Catheterization. I thought I'd include a link to a YouTube video that shows how this device is used:
Although the device has advance considerably since then (see below), the images it provides are still pretty much the same.
I will often use the device to locate and mark an internal jugular vein before draping the patient as I find the use of the needle guide extremely cumbersome.
[Site-Rite]
Tight Brain Checklist
-
Printer Friendly|#| Trackback
The anesthetist can have a significant impact on the operating conditions a neurosurgeon has to work with. One example is a situation where the surgeon (or anesthetist) notices the brain no longer appears relaxed but begins to get 'tight' within the craniotomy window. Rather that a knee-jerk response of further hyperventilating the patient and/or giving Mannitol, it is prudent to first consider possible causes as follows:
- Are the pressures controlled?
- Is the metabolic rate controlled?
- Are vasodilators in use?
- Are there any unexpected mass lesions?
Are the pressures controlled?
- Arterial Pressure
- pCO2
- pO2 (remember that hypoxemia is a potent stimulus for cerebral vasodilation
- Intrathoracic pressure
- Airway pressure
- Jugular venous pressure (includes external venous compression by C-spine collar or twill used to secure endotracheal tube)
Is the metabolic rate controlled?
- Pain
- Light anesthesia
- Awareness
- Seizures
Are vasodilators in use?
- Potent agents (Isoflurane, Desflurane, Sevoflurane, Enflurane)
- Nitroprusside
- Nitroglycerine
Are there any unexpected mass lesions?
- Pre-existing pneumocephalus exacerbated by nitrous oxide
- Cerebral hemorrhage remote to the site of surgery
As taught to me by John Drummond, M.D. at UCSD
Pandora's Box Of Music
-
Printer Friendly|#| Trackback
It looks to me like this would solve the OR's music problems. Staff could pre-program their favorite station and just log in from an operating room computer...as long as that wouldn't interfere with online shopping...

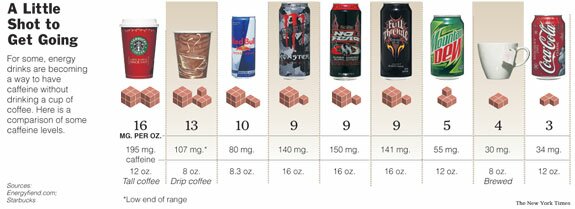
How much caffeine does that drink have?
-
Printer Friendly|#| Trackback
I've written before about caffeine addiction in surgical patients. In recent years there's been an explosion of caffeine-containing beverages. Having some idea of the caffeine content of the major ones can help you choose an appropriate dose.
The Energy Fiend web site has a nice Caffeine Database. I found it via a recent NYT article.
How To: Awake Fiberoptic Intubation
-
Printer Friendly|#| Trackback
This definitely falls in the "don't try this at home" category, but if this technique is different than the one you use, give it a try. It will surely result in a net gain in style points.
How To Do An Awake Fiberoptic Intubation
Technorati Tags: Anesthesia